| |
| |
| |
| |
 母亲晚期肺癌跨越11年了!我们的5点
讲述者:小白兔整理者:pear
2014年母亲确诊晚期肺腺癌,一路摸索抗癌前行,幸得病友
母亲晚期肺癌跨越11年了!我们的5点
讲述者:小白兔整理者:pear
2014年母亲确诊晚期肺腺癌,一路摸索抗癌前行,幸得病友
 国产肺癌新药获批上市!疾病控制率98
作者:seacat
5月29日,国家药品监督管理局(NMPA)通过优先审评审批程序附条件批准瑞
国产肺癌新药获批上市!疾病控制率98
作者:seacat
5月29日,国家药品监督管理局(NMPA)通过优先审评审批程序附条件批准瑞
 治疗对肿瘤的有效率超过90%,晚期肺
作者:Tony
鳞状细胞癌起源于上皮层,是一种常见的癌症病理类型,多见于肺癌、食管癌
治疗对肿瘤的有效率超过90%,晚期肺
作者:Tony
鳞状细胞癌起源于上皮层,是一种常见的癌症病理类型,多见于肺癌、食管癌
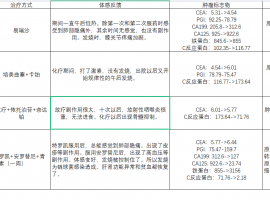 SMARCA4-NSCLC 盲试靶向药有效!!
首先感慨一下今天真的是个好日子。努力了进三个月的治疗终于有了重大进展。
复查结果
SMARCA4-NSCLC 盲试靶向药有效!!
首先感慨一下今天真的是个好日子。努力了进三个月的治疗终于有了重大进展。
复查结果
 老公刚刚54岁,确诊肺癌,手术中发现
各位朋友好。
度过了慌乱的一个月,有机会发现了这个论坛,如获至宝,说说我家
老公刚刚54岁,确诊肺癌,手术中发现
各位朋友好。
度过了慌乱的一个月,有机会发现了这个论坛,如获至宝,说说我家





 显身卡
显身卡


