本帖最后由 滴水 于 2013-4-17 17:27 编辑
5 t* E; t& I2 c3 N* r6 C( Z6 V$ G+ j; `7 G" f
1. CP化疗联合低剂量口服cediranib,能提高反应率 (52% vs 34 %),但OS和FFS无区别,另外毒性反应会增加;是否提示凡德和化疗联合,也能提高反应率?$ h/ P5 k. x- o& J7 D
http://www.asco.org/ASCOv2/Meeti ... mp;abstractID=98578/ T* }" b3 ~7 e) O6 |
6 N |# z* ?7 g; o) A' @
2. 多线治疗的NSCLC, xl184 100mg qd ,结果:0RR(CR+PR) 10%,肿瘤有退缩的64%
6 K4 }+ n+ T% l! L2 ghttp://meetinglibrary.asco.org/content/95281-1142 m* Y; u9 G7 h5 x/ O( C
第一次特3个月就耐药,其中第一个月联合了12天 xl184,效果最明显,会不会其实是XL184在起作用?
G- N) b4 N: F9 j: e2 q7 t& w" X- g. |. ^7 `' X8 \% y$ u
3. 野生和非野生的T790M突变+ L* {: s% t k! C$ J" R) _& {# f
Results: The T790M mutation was detected in 21/64 (32.8%) p in the erlotinib arm and 26/59 (44.1%) in the chemotherapy arm. PFS was 12.1 m for p with mutant T790M in the erlotinib arm, 8.8 m for p with wt T790M in the erlotinib arm, 6.3 m for p with mutant T790M in the chemotherapy arm, and 4.5 m for p with wt T790M in the chemotherapy arm (P<0.0001). OS was not reached for p with mutant T790M in the erlotinib arm, 16.1 m for p with wt T790M in the erlotinib arm, 22.6 m for p with mutant T790M in the chemotherapy arm, and 18.4 m for p with wt T790M in the chemotherapy arm (P=0.04). Conclusions: Our unexpected finding that p with EGFR compound mutants attain the maximum benefit from erlotinib suggests a need for more sensitive assays to detect EGFR compound mutants and for studies of inhibitors targeting the EGFR T790M mutation. Whole genome sequencing may provide greater understanding of the genetic factors involved in the differences in OS.
2 K2 {$ d2 G4 r( |& b) M
3 T! V0 C0 u, c5 Q4 M4 m4. EGFR-TKI耐药后,继续联合化疗,比单独化疗应答率要高(41% vs 18%) ]5 o) @7 p5 M& T
http://www.asco.org/ASCOv2/Meeti ... mp;abstractID=98539
8 g5 n2 G A0 \: ~! s
8 S. _1 L+ u+ J2 i2 L+ m& F5. EGFR-TKI耐药后,间隔一段时间重新服用,仍有一定的有效率
`. m" I0 ?' t( ^6 K/ e# Ohttp://www.asco.org/ASCOv2/Meeti ... mp;abstractID=94857: z* Y9 J" C# K5 O3 v7 [/ J
b+ l% } z# k; x0 m" l6. 有T790突变的EGFR-TKI耐药,进展比较慢+ b2 X% e# c+ `! v7 R" u
# b# C- n3 x, i; i- ]
' M H7 J/ @4 B8 f0 A% ?
3 [9 p2 |. Z! E' Y% \3 P: ~9 K5 U |
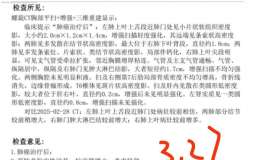
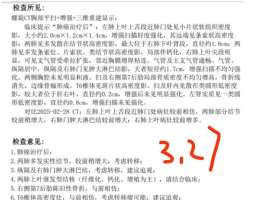 一线三代29个月,四次培美加卡铂出现
患者信息:女,57岁。确诊时肺内广泛转移+脑部多发转移+肝部转移+骨转移。组织检测600
一线三代29个月,四次培美加卡铂出现
患者信息:女,57岁。确诊时肺内广泛转移+脑部多发转移+肝部转移+骨转移。组织检测600
 母亲晚期肺癌跨越11年了!我们的5点
讲述者:小白兔整理者:pear
2014年母亲确诊晚期肺腺癌,一路摸索抗癌前行,幸得病友
母亲晚期肺癌跨越11年了!我们的5点
讲述者:小白兔整理者:pear
2014年母亲确诊晚期肺腺癌,一路摸索抗癌前行,幸得病友
 2026年将有哪些肺癌新药有望纳入医保
作者:seacat2025年国家医保目录谈判即将开始申报。那些在国内获批上市但未进入医保目
2026年将有哪些肺癌新药有望纳入医保
作者:seacat2025年国家医保目录谈判即将开始申报。那些在国内获批上市但未进入医保目
 23年脑膜转,目前脑部稳定,肺原发灶
2025.3至2025.5.22脑实质和脑膜稳定,肺部原发灶及胸腔积液控制不住。CEA持续升高。
23年脑膜转,目前脑部稳定,肺原发灶
2025.3至2025.5.22脑实质和脑膜稳定,肺部原发灶及胸腔积液控制不住。CEA持续升高。
 男77周岁 肺腺癌 2018年右上肺切除
父亲77岁 2018肺腺癌右上肺切除,今年6月份增强CT检查报告(右上肺术后,术区见金属缝
男77周岁 肺腺癌 2018年右上肺切除
父亲77岁 2018肺腺癌右上肺切除,今年6月份增强CT检查报告(右上肺术后,术区见金属缝





 显身卡
显身卡 * l. d+ ~2 `2 v+ w% k1 k
* l. d+ ~2 `2 v+ w% k1 k